About anal fissure
An anal fissure is a small tear in the lining of the anal canal, usually caused by trauma such as passing hard stools or repeated diarrhea. It often presents with sharp pain during or after bowel movements, sometimes with bleeding. Chronic fissures may persist for months and can become resistant to standard treatments such as ointments, dietary adjustments, or even procedures like Botox injections.
Patient background
The patient, a 72-year-old male, developed an anal fissure following a course of antibiotics that caused severe diarrhea. Conventional management included topical ointments and a recommendation for Botox injections. He was also advised to eat bran, which worsened the condition by inducing constipation.
- Vegetarian since age six.
- Prior history of anal fissure about 20 years ago.
- At presentation: three months of ointments with only slight improvement; ongoing severe pain with bowel movements and bleeding.
Treatment course and points used
The patient began treatment twice weekly for four sessions, then continued once weekly.
- First treatment: Bloodletting in the occipital area of the leg — a key zone for anal disorders such as hemorrhoids and fissures.
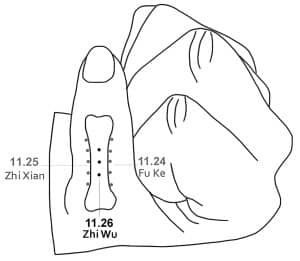
- 11.26 Zhi Wu: Used consistently for wounds that fail to heal, until bleeding stopped.
- 33.01–02 San Qi and Yao Ling: Main points for treating the fissure.
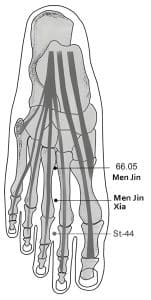
In some sessions, San Qi was needled with six needles: two needles at the same point, one inserted vertically and the other more superficially (see image). - 66.05 Men Jin, 77.11 Si Hua Xia, 77.12 Fu Chang: To regulate the intestines and relieve constipation.














Progression
- After 8 treatments: Bleeding stopped, though pain during bowel movements persisted.
- After 10 treatments: Three consecutive pain-free days.
- After 11 treatments: Pain reduced to only one day.
Turning point
- 13th treatment: The fissure-related points that had been used were no longer active. I therefore searched for additional active points and found Liu Shui active bilaterally, so I included them.
- 14th treatment: Following the addition of Liu Shui, the patient reported significant improvement — almost no pain.
- 15th treatment: A proctologist confirmed complete healing of the fissure, leaving only a small scar.
The patient continued with maintenance treatments to preserve the outcome and prevent recurrence. Point selection was adjusted at nearly every session, guided by VAS assessment to determine activity and whether to needle unilaterally or bilaterally.
Liu Shui points (six water)
These are relatively lesser-known points first introduced by Hu Wen Zhi.
Location (6 points):
- Shui Zhi – Located 2 cun lateral to the tip of the medial malleolus and 6 cun proximally; 1 cun above Ki-9 (Zhu Bin).
- Shui Ming – 1 cun above Shui Zhi.
- Shui Qing – 1 cun above Shui Ming.
- Shui Zhen – 1 cun above Shui Qing.
- Shui Yin – 1 cun above Shui Zhen.
- Shui Quan – 1 cun above Shui Yin.

Reaction area: Kidney, Six-Fu.
Clinical application: Reported to be effective for hemorrhoids and hemorrhoidal bleeding. Points that treat hemorrhoids may also be applied to anal fissures; in this case, adding Liu Shui marked the clinical turning point.
Clinical reflection
This case underscores the value of treating based on active point selection rather than following a fixed protocol. The gradual improvement and decisive shift after adding Liu Shui highlight the importance of dynamic, VAS-guided point choice.
For more information about the VAS.
For more detailed information about these points, download the Master Tung’s Points app


